Introduction
Catheter ablation (CA) represents a valid treatment option in patients with drug-refractory symptomatic atrial fibrillation (AF). The majority of catheter ablation trials have mainly enrolled patients with preserved LVEF and paroxysmal AF. However, a significant number of patients with AF also have heart failure (HF) and rhythm control with antiarrhythmic drugs has not shown satisfactory results in randomized trials both in patients with or without HF. Whether CA is superior to Amiodarone (AMIO) for the treatment of persistent AF in patients with HF is unknown.
Material and methods
This was an open-label, randomized, parallel-group, multicenter study. Patients with persistent AF, dual-chamber ICD or CRT-D, NYHA II-III and LVEF < 40% within the last 6 months were randomly assigned (1:1 ratio) to undergo CA for AF (group 1 = 102 patients) or receive AMIO, (group 2 = 101 patients). The main goal of the ablation procedure was pulmonary vein antrum isolation. Recurrence of AF was the primary end point. Recurrence of AF was the primary endpoint.
Results
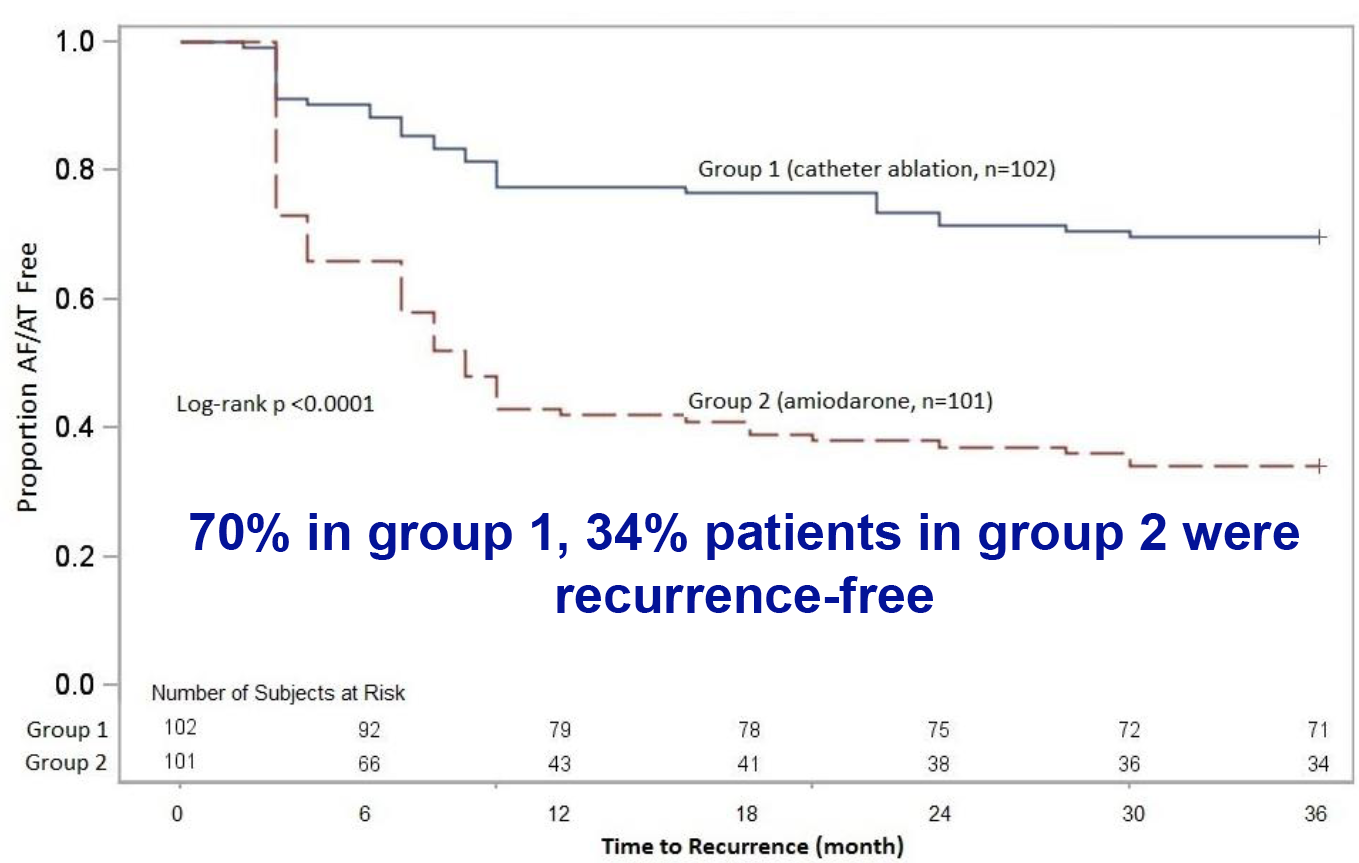
Baseline characteristics were not different between groups. At 26 ± 8 months follow-up, 71 (70%) patients in group 1 were free of recurrences after average 1.4 ± 0.6 procedures as compared to 34 (34%) in group 2 (log-rank p < 0.001). Success rate of CA in the different centers after a single procedure ranged from 29% to 61%. After adjusting for covariates in multivariable model, patients on AMIO therapy were found to be 2.5 times more likely to fail (HR 2.5 [95% CI 1.5 to 4.3], p < 0.001) compared to CA. Over the 2 year follow-up, hospitalization rate was 31% (32 patients) in group 1 and 57% (58 patients) in group 2, p < 0.001, showing 45% relative risk reduction (RR 0.55, 95% CI 0.39-0.76. A significant lower mortality was observed in CA (8 [8%] versus AMIO (18 [18%], p = 0.037).
Conclusions
This multicenter randomized study shows that CA of AF is superior to AMIO in achieving freedom from AF at long-term follow-up and reducing hospitalization and mortality in patients with heart failure and persistent AF.





